
A4
Staff
Survey.
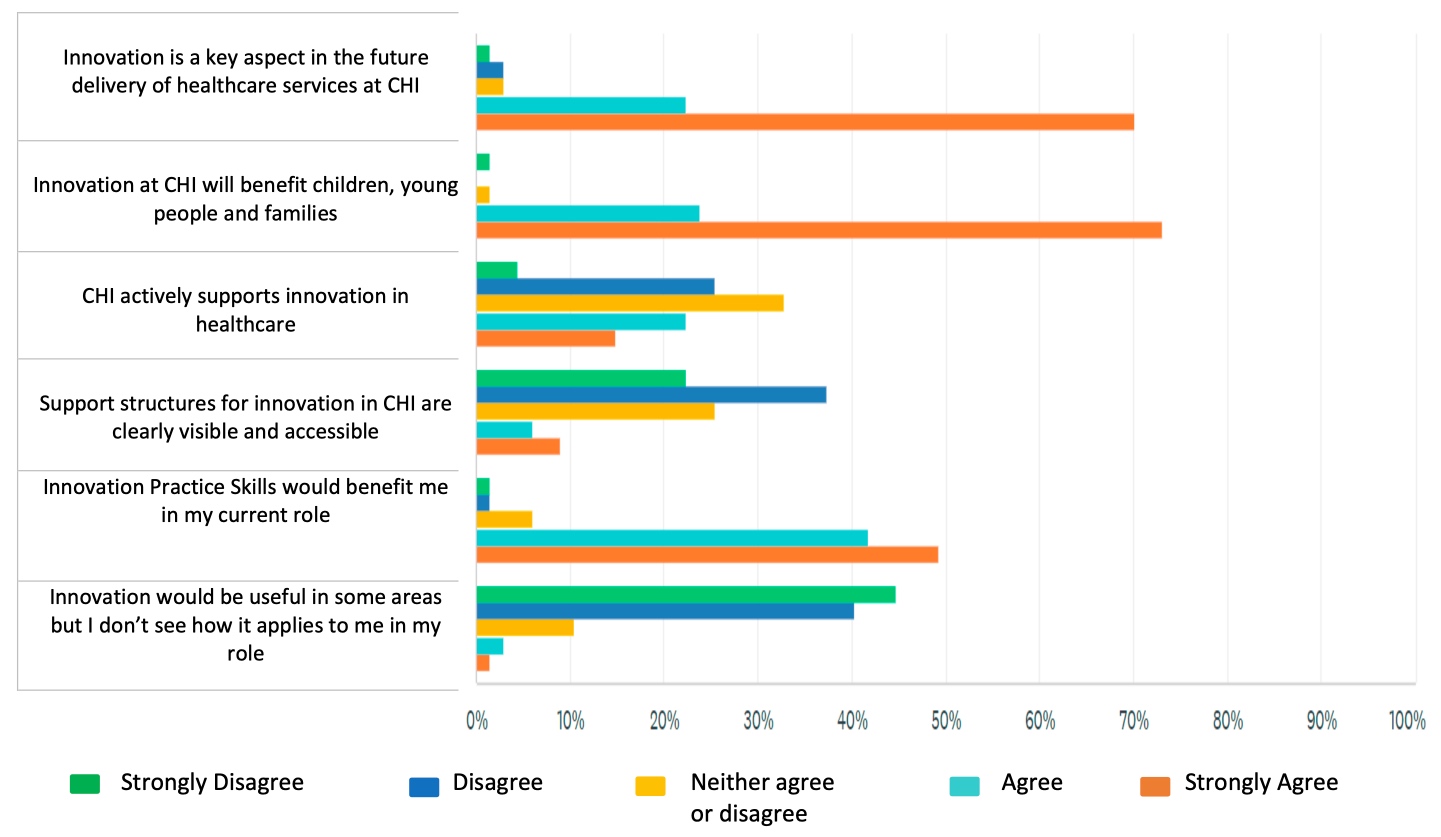
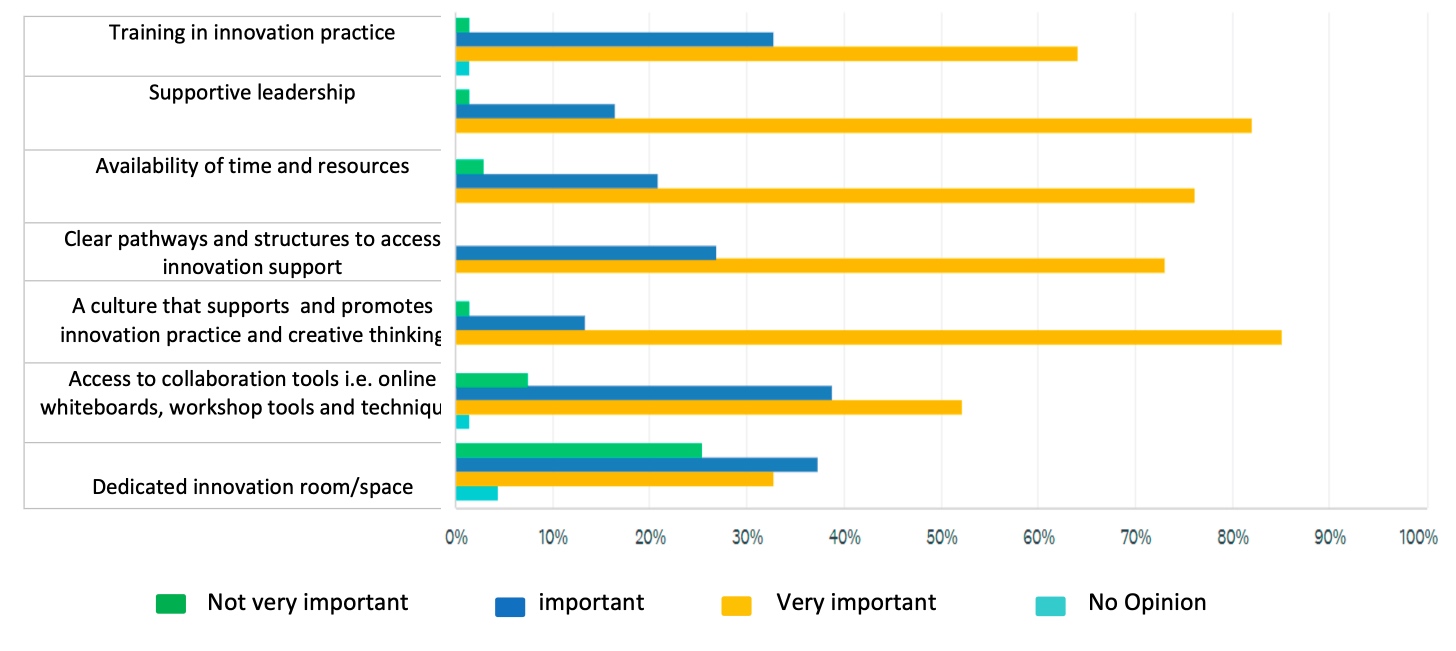
We surveyed CHI staff to get a sense of their views on innovation in CHI and understand more about their current experience. The full breakdown of responses is included below. In general, the responses showed a strong support for innovation practice with 93% either agreeing or strongly agreeing that innovation should be key aspect of the future delivery of healthcare services at CHI. The vast majority considered innovation as relevant to their current role. More than half of the respondents had no experience of being involved in innovative projects and only a small number had undertaken training or education relating to innovation; however, they welcomed opportunities for further training and support. The largest barrier to innovation was perceived as time and resources, with culture and leadership coming out as the most
Benchmark Sites and Interview Participants:
Q1
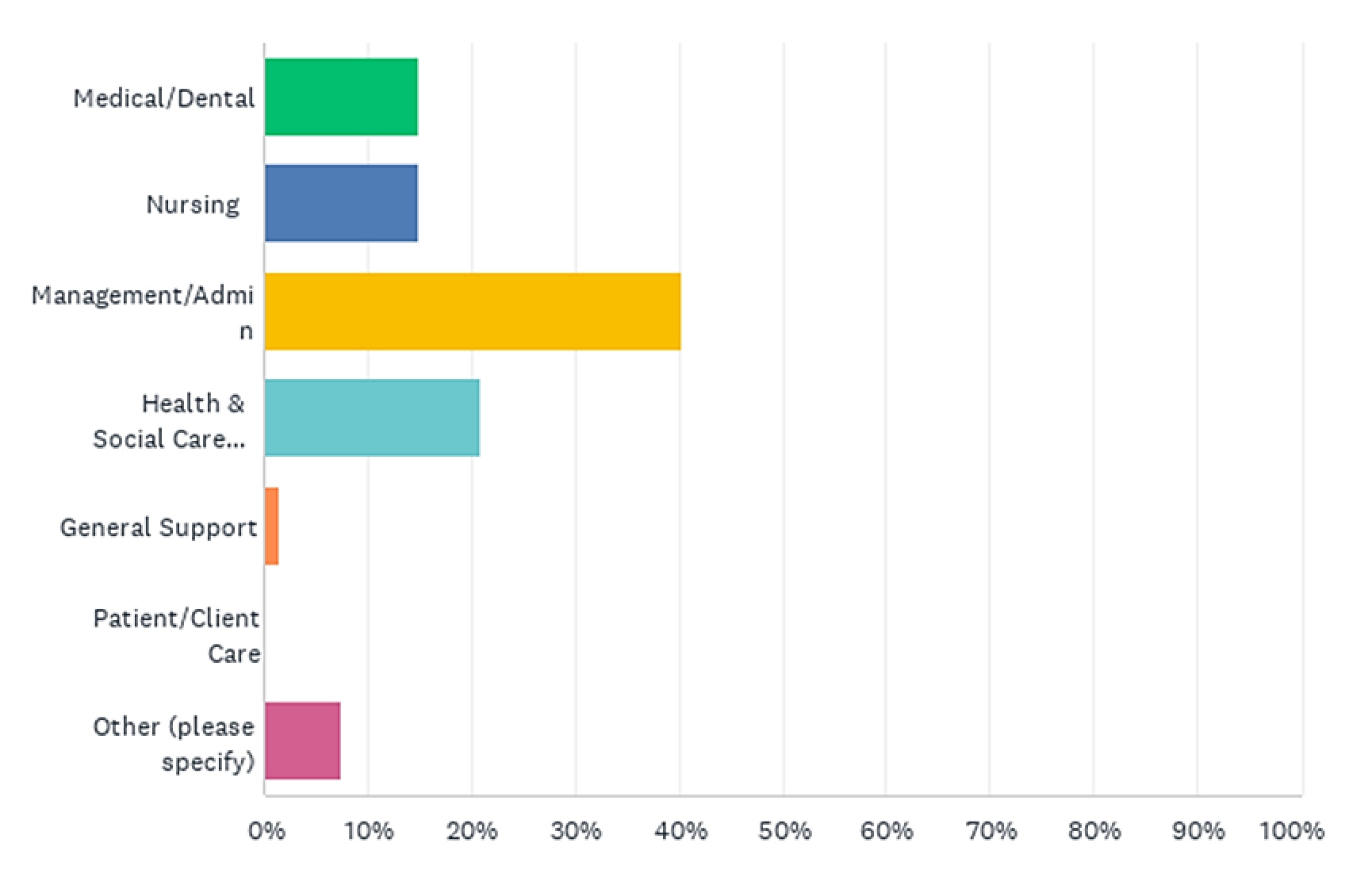
Which HSE Staff Category Best Describes Your Role?
Q2
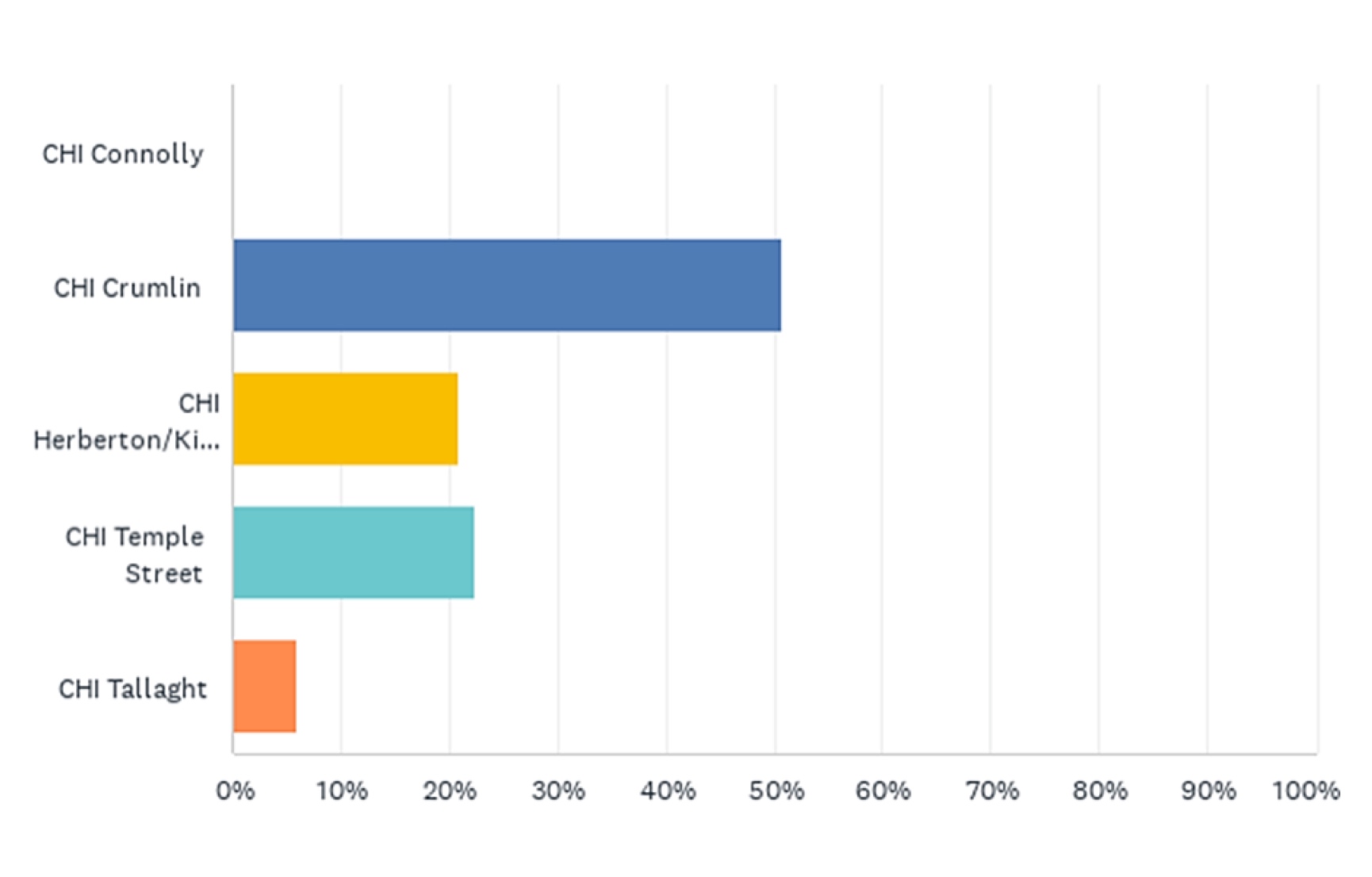
Where Are You Principally Based?
Q3
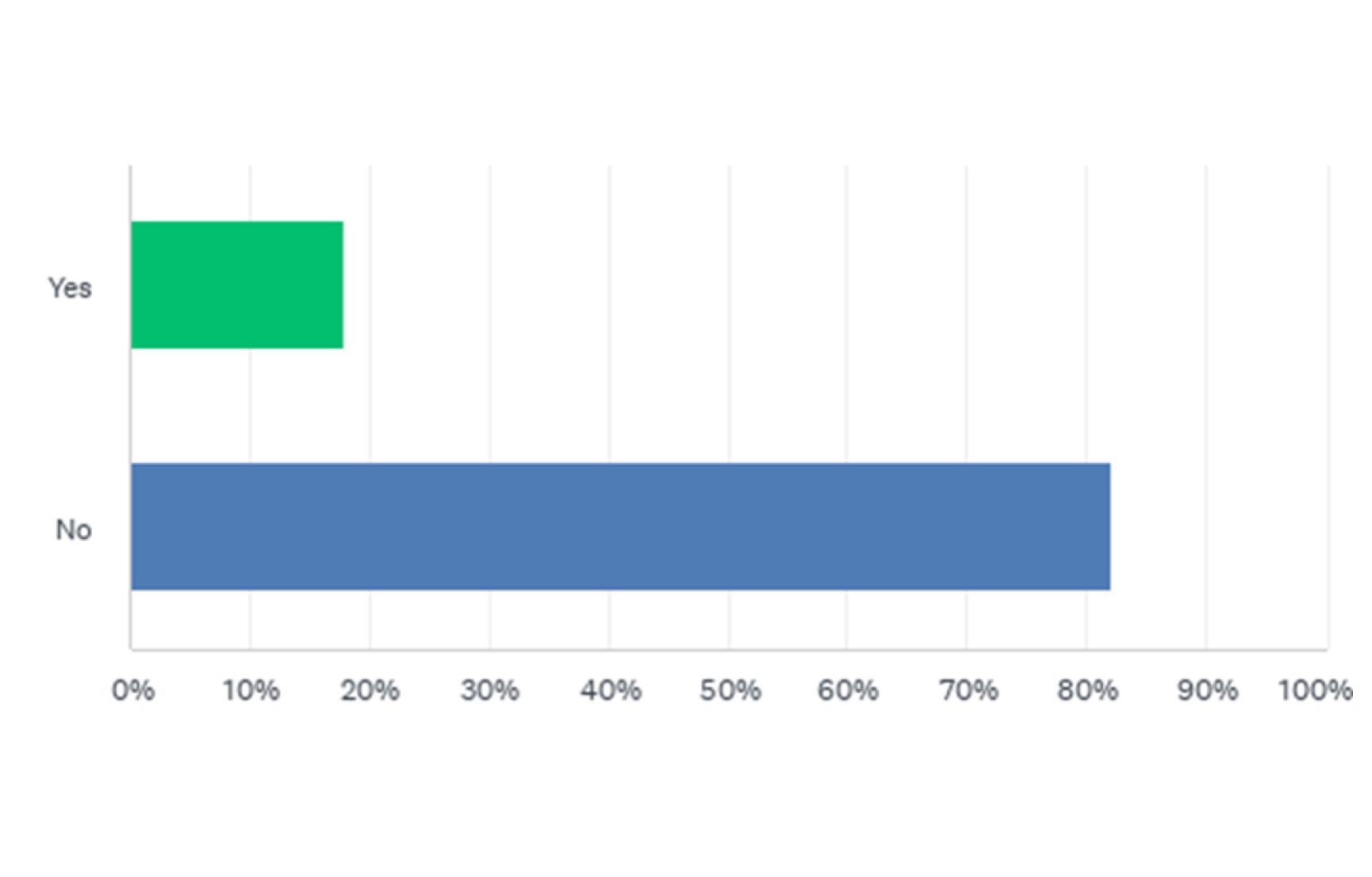
Have you completed training/education relating to Innovation/Innovation Practice?
Q4
If yes, please give further details:
- Translational research to PhD
- I am taking one at the moment as I finally got an opportunity to take trainings I have been waiting for! It’s great. Thank you very much.
- Post graduate degree level
- RCSI NHS
- Part of Master Degree
- Lean Healthcare Quality Management Lean Six Sigma
- I have developed videos which have had >1 million views on YouTube
- D4AHS – virtual Design Labs in Healthcare – Human Centred Design. – Transformation Academy for Large Scale Change. – S4CA NHS Horizons.
- PhD. Currently studying is in Artificial Intelligence and Software Innovation
- Lean Six Sigma
- UCD Diploma in Innovation, creativity and leadership
- MSc Education – E-learning MSc Cyberpsychology MA UX Design Process and interactive technologies (completion date August 2022)
Q5
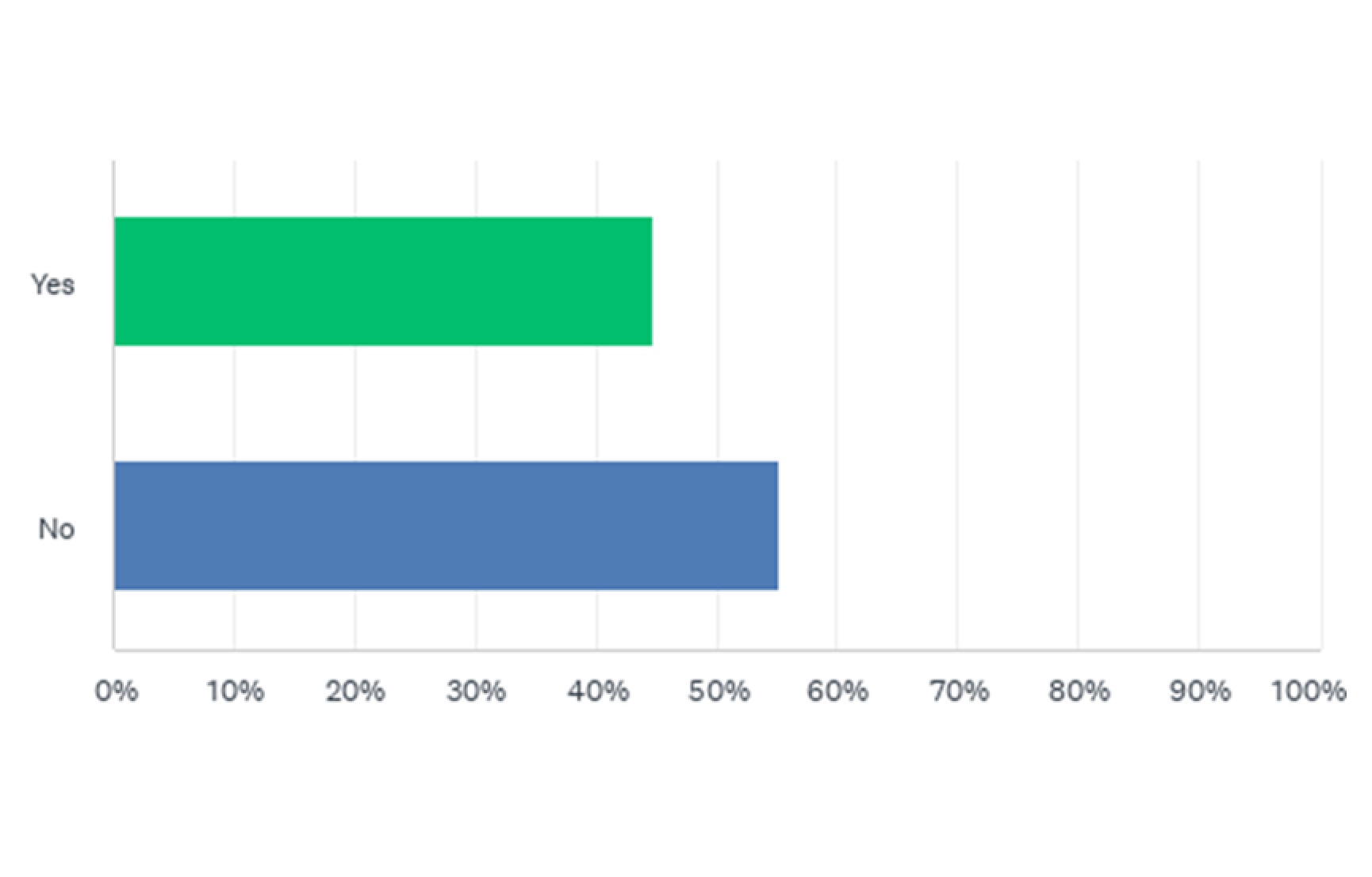
Have you completed training/education relating to Innovation/Innovation Practice?
Q6
If yes, please give further details:
- Setting up a new nursing service
- Developing new clinics, new clinic modalities, NTPF initiatives
- Tiny little projects at departmental level – unsupported and not great. We needed more help!
- Smart-pump implementation, expansion of paediatric formulary to new platforms/locations across CHI
- Accessing lab results from other hospitals remotely here in Crumlin using existing Healthlink platform
- Saturday Clinics Food Challenges City West Establishing Attend anywhere clinics in Crumlin Creating special Covid safe clinics Bleep to Sleep project Cross site Anaphylaxis video Email support for national Covid Vaccines sites
- HSE Rainbow Badge, CHI Professionalism
- Tele medical service development
- Redesign of department to increase clinical space
- LOS reduction times initiatives around patient outcomes (first time trail at CHI)
- e-Learning systems, innovations to improve HR SOP
- Multiple world class research projects, ongoing paediatric drug book for Ireland (awaiting PID execution), Intubation checklist and airway trolley across CHI, Ultrasound for PED
- I am currently co-leading an innovative project: Music Therapy assisted Dental procedures for children with complex medical needs.
- Variety of Clinical services, inc development of the initial concept of the 2222 system in Ireland. stock management- Lean stock management in Cath lab -concept further rolled out by Joe Ellis when he came to Crumlin, Coms services and reportage. Patient self-booking systems (swiftqueue’s introduction to Crumlin). Introduction of 3D modelling in clinical buildings and services design and consultation with users – later copied in NPH design/consultation processes – Navis works. Clinical education systems – live links between HCCL and lecture theatres in USA and France. Give a man a fish, feed him for a day, teach a man to fish feed him for life- thus bringing the skills of the team in Ireland out to the world. Clinical waste management & education – basically lots of crowning the customer innovations over the years since I 1st “temporally” came in here to set up the 1st Clinical genetics service based in a paediatric hospital over 25 years ago
- I have liaised with Barry McMahon to do workshops with patient involvement to try and automate our triage process
- Predominantly QI focussed projects at departmental/clinical level.
- Whilst in Temple Street, I developed several bespoke applications some of which include the following: 1. Nursing handover System 2. Outpatient appointment text messaging and patient response mechanism to handle DNAs. 3. Docuport – Application to allow clinical departments easily convert their paper reports to digital format. 4 LabScan – Mechanism to allow external lab reports get scanned and auto inserted as a link within their lab software 5. Several Excel to Web-based data entry applications
- Robotic Process automation Automation of NTPF uploads
- While traditional in overall approach, the EHR programme at CHI is seeking to enable the transformation of the ways of working of all clinical staff, through innovative use of technology to improve patient experience and outcomes.
- N/A BUT WOULD LOVE TO HAVE THE OPPORTUNITY TO GET INVOLVED
- Clinical Operating Models in 2017/2018/2019
- Community Benefit Programme
- Designing and building interactive touch screen content for children in Temple Street OPD Designing and building eLearning modules Temple Street Designing and producing video content for Digital Signage in Temple Street and Connolly Managing Digital Signage in Temple Street and Connolly – three separate systems Responsible of Social Committee tile on MyChi
- PMO support
- Waiting list
- Like waste management
Q7
Please rate your level of agreement with the following:
Q8
In your opinion, please rate the following in terms of how important they are for supporting and enabling innovation:
Q9
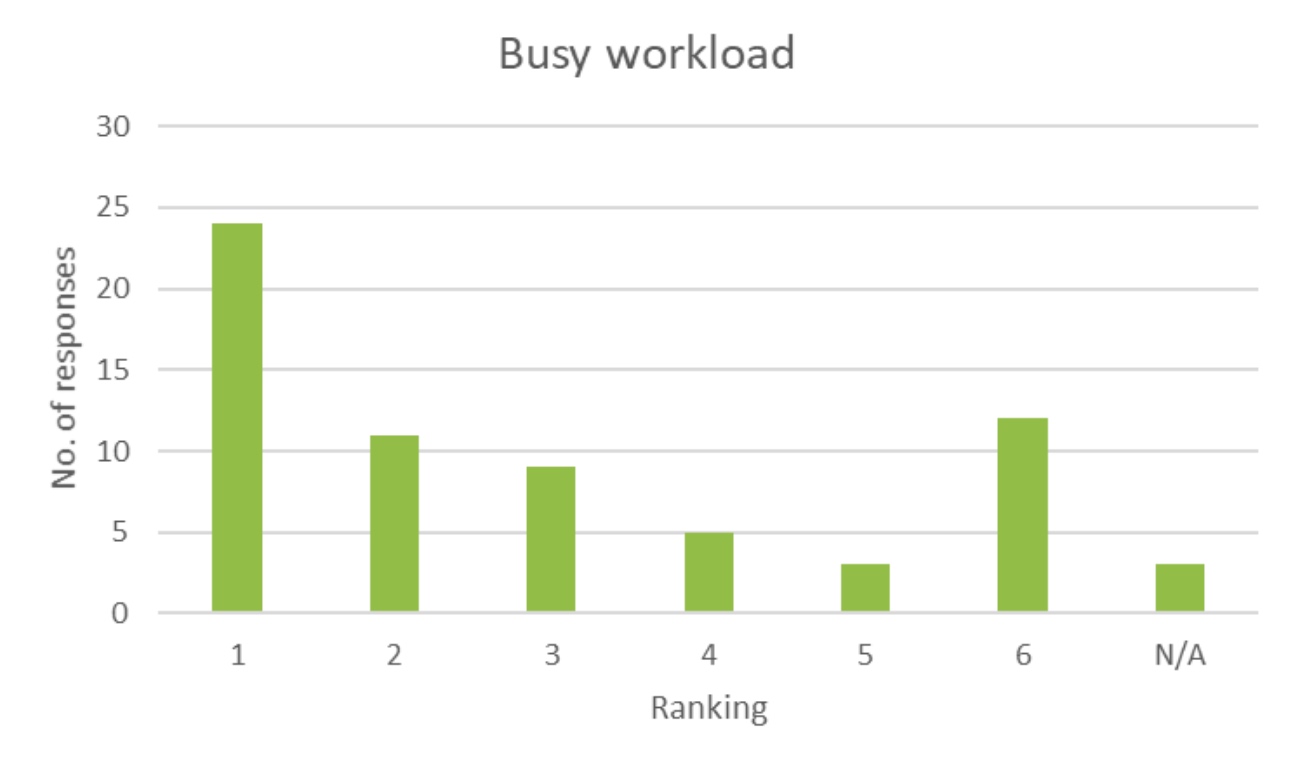
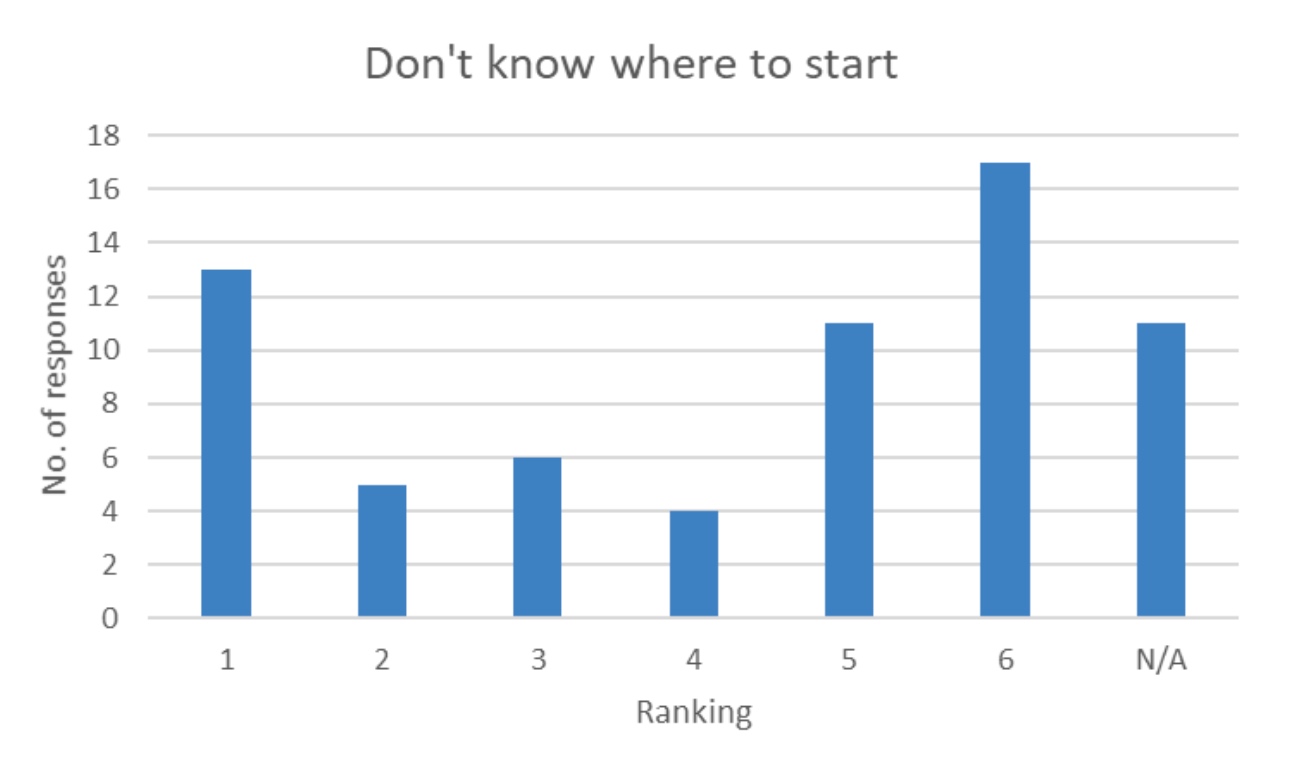
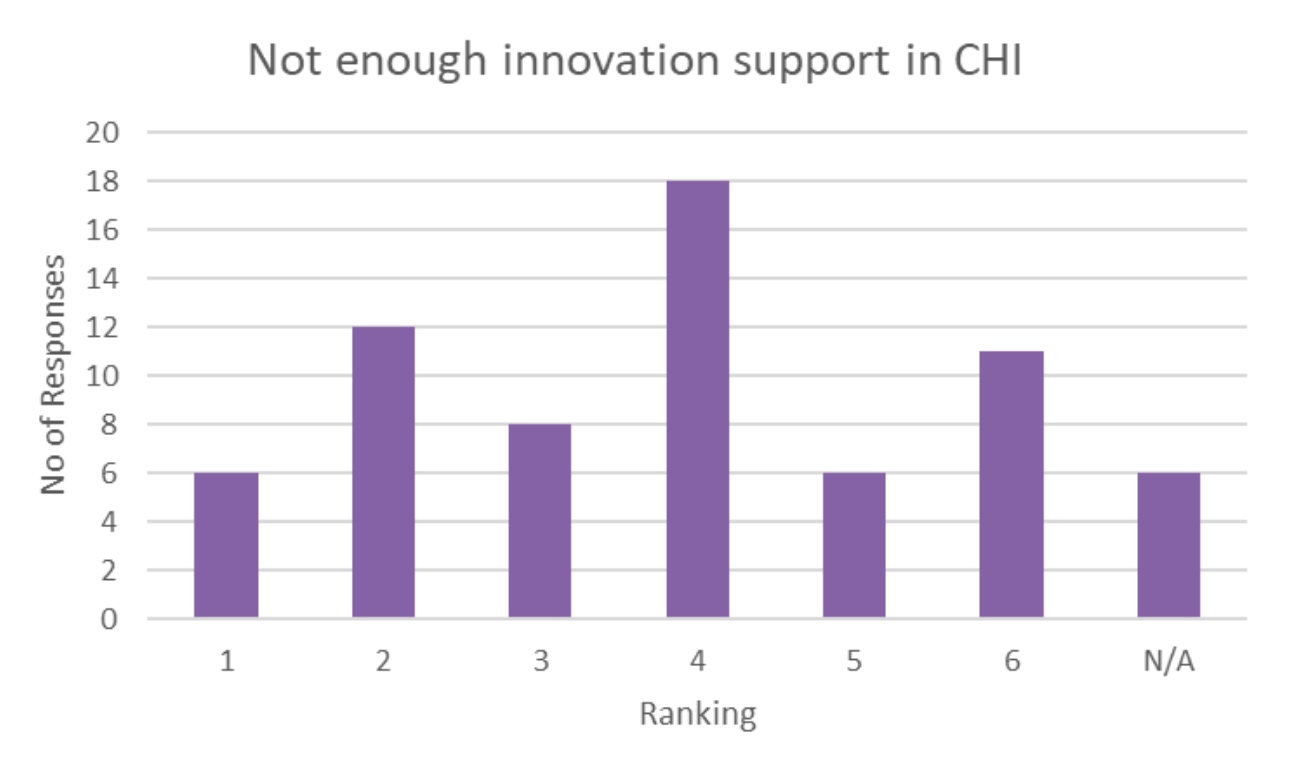
What would you see as the most likely barrier to you engaging in innovation activity in your current role
(Rank 1-6: 1=greatest,6=least):



Q10
In thinking about an Innovation strategy for CHI, do you any other thoughts or comments?
- Long overdue, it’s a very welcome start but must be encouraged from ground level upwards. there are lots of people with great ideas who need encouragement and support to bring forward ideas
- Just ask their views and start conversations please.
- I think that as high performing healthcare professionals we are “bred” to find failure unacceptable. This can stop us from being comfortable in experimenting and being creative. It is so well known in the creative sector that the process of creation involves failure in order to improve and develop a final piece. As HCWs, failure goes against the grain. This requires a cultural shift.
- The non-mention of research innovation here is concerning. Otherwise this will be a lightweight entity within CHI that will not be taken seriously internally/externally.
- Need specific resources and important to be cross site. Need the basics improved upon first. I.e. not enough computers, not enough phones or very old technology at present, and minimal resources or ability for remote working. Different systems used across CHI meaning information transfer is a huge barrier.
- NCHDs are generally an overlooked group when it comes to innovation. Many have worked abroad and have experienced foreign healthcare systems. Engaging these NCHDs would be a great way to use this experience to better the care we provide. Workload is an issue for most NCHDs but in my experience most are really willing to share their experience if asked
- Flexibility to allow rapid role out of projects especially during emergencies: COVID/ Cyber-attack. This is when innovation is needed most…learn as you go instead of endless preparation. Innovation leads (go to people) in areas that the clinical staff have less contact: procurement, building, supplies. A massive increase in IT support for innovative digital projects.
- I don’t think a physical space is necessary especially during the pandemic. An online interactive platform would suit the times we live in now and beyond.
- No support whatsoever for innovation in CHI at Temple street, any projects that can seek funding need to have a consultant associated with them which is not always possible
- Clinical governance needs to be teased out from project management or innovation development as are not the same thing but many initiatives are at risk of being blocked by clinical leaders working very hard but with less interest in creative or systems thinking.
- It’s a good idea but without supports for staff initially through a better place to work it is futile. Staff are deflated, mental health is at an all-time low and staff just want to get in do their job and go home. It is a great idea just at the wrong time
- I believe innovation should permeate every aspect of our daily work. It is only by constantly peering above the parapet of possibility that we as a whole can advance care and service delivery for all we work for.
- Communication, culture and leadership support is crucial for innovation strategy.
- I think this is so vital not only for how we work more effectively and efficiently but it is SO important for retention of staff and attraction of staff. We are continuously firefighting with no strategy and innovation should do hand in hand with strategy. We are aiming for a digital hospital and yet we don’t have a communicated strategy for business or specifically in my area no strategy at all!
- The archaic financial structure, hospital politics, the idea that only consultants can be heard, and very poor IT infrastructure are some of the many things that hinder innovation
- There are multiple big projects in PEM that need support. Can you start with them? First up the paediatric emergency drug book.
- Wouldn’t it be wonderful if there was a certain staff member who you could contact for support and guidance about getting an innovative project up and running? At present the only method that I am aware of to fund innovation comes from the foundation. Having a hospital budget would be wonderful with an application process to ensure high quality outcomes from the service.
- Every member of staff has a contribution to make. Encourage them do not exclude them. Current ways of communication in CHI exclude staff that do not have access to IT many do not even have e-mail. They are excluded from many communications. Invite people in to communicate, let them know their input is valued.
- Neglect of IT systems results in clinical risk, I spend hours every week triaging because innovation never happens, its talked about but the lack of action is shocking
- Innovation requires good ideas, thinking outside the box, the ability to see how things can be done better for patients and resource to drive positive change. A proactive rather than reactive culture needs to be created in CHI to deliver innovation.
- Invest in appropriate collaboration technology, once and for all. Reduce cumbersome governance, at least a little to allow for agility.
- As per other written comments- I worry that the use of the word ‘innovation’ would be off putting to many before they would even delve into understanding what it might mean. Innovation may suggest connotations of really new novel care/therapies etc. While CHI will hopefully support that too the notion of improvement or even transformation of service may invite more interest. The research survey circulated previously appeared to be only concerned with clinical trial research & PIs. I understand Innovation to be a sub division/sit within research? Is Education (HEI) considered a separate strand again? & L&D separate under HR? & QI under QRSM? & Change only a programme lifetime! There are so many highly motivated CHI staff (myself included) interested in change & improvement but no singular unifying strategy (function/department) that draws all tribes together with a common focus (I’m thinking Pillar Centre type umbrella) Probably muddled thoughts as I sign off for Christmas- delighted to see dedicated resources for this in CHI & hoping that your strategy & influence will unify healthcare transformation approaches in CHI under a singular umbrella.
- The people I’m dealing with in the base hospitals are too busy dealing with the day-to-day to even think about innovations that might save them time.
- A centre of Innovation Excellence needs to be established, where research teams can submit ideas to develop into projects
- Approved outside training
- The best innovations will happen across organisational boundaries. It would be good to purposely bring interested reps from each organisation and location together to brainstorm collaborative innovation ideas.
- Collaborative projects
- just that I would love the opportunity to get involved. Very excited about the future of CHI.
- It would be super if there were regular training days for staff.
- A basic course – on HSEland, for example – explaining what innovation is and how it might look at CHI – would be a very helpful start.
- Need Lean Management approach for Corporate Functions including Operations and for Management and Admin in particular.
- Currently enrolled in a Healthcare Innovation course, it has broadened my view on healthcare innovation opportunities but I feel they are given to those more so in upper management rather than frontline. Frontline staff should be encouraged and given protected time to access and engage with resources available. Many innovative opportunities can be discovered if discussed with frontline staff however can get missed because they don’t have time to voice their opinion to the right people.
- I hope that CHI is looking to local partners both within and outside healthcare in Ireland for support in this. A lot of the transferable skills required to design and implement this strategy are available nationally and I hope that we’re not trying to reinvent the wheel when other institutions have successfully implemented such. I would also like to see more inclusion of both patients’ families and non-permanent staff (including NCHD’s) included in the implementation of this strategy. Sometimes it needs those who are less embedded in the system to recognise opportunities for innovation and I think those voices are often unheard in CHI structures.
- Support from management is the main reason we should get first before taking further steps.